For cancer patients, a diagnosis is generally followed by staging. Among other things, the stage of a cancer tells the patient and physician if the cancer has spread and if it’s metastasized to the lymphatic system or other organs, etc. This information is used to determine the course of treatment (i.e. whether the cancer is operable or not), as well as prognosis (predicting a patient’s survival time). For scientists, this classification is also helpful in a research setting as it allows comparison of patients (simplistically, it allows them to compare apples to apples.)
TNM is the staging system generally used in pleural mesothelioma (peritoneal mesothelioma doesn’t have a staging system). It is described in the American Joint Committee on Cancer (AJCC) publication on staging systems, and is based on three pieces of information, which can be even further broken down:
T: the extent of spread of the main tumor.
N: the spread of cancer to nearby (regional) lymph nodes.
M: indicates whether the cancer has spread (metastasized) to other organs of the body.
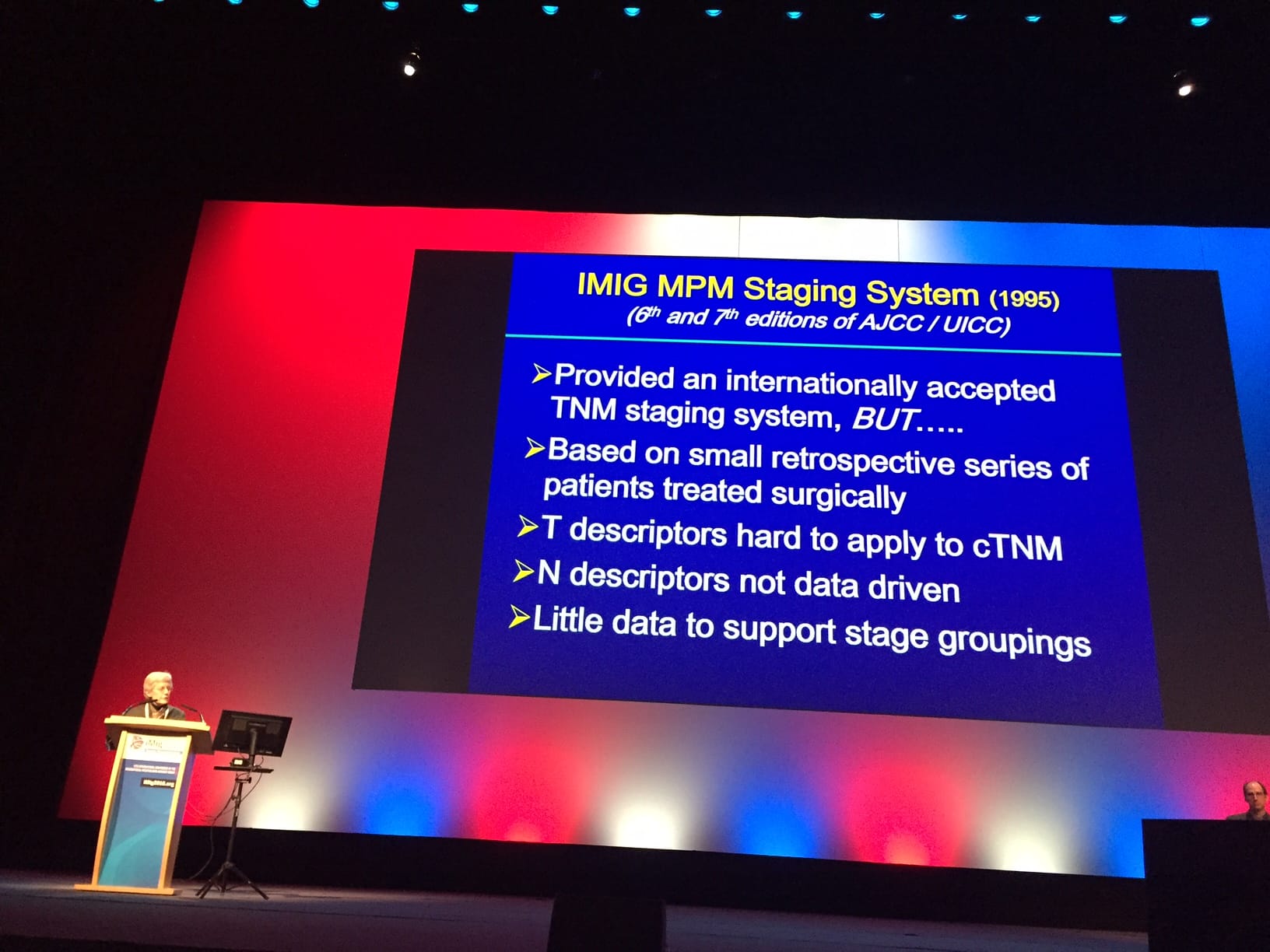
Currently, this staging system for mesothelioma is undergoing a review and update, an effort partly funded by the Mesothelioma Applied Research Foundation, and is scheduled to take effect in early 2017. Dr. Valerie Rusch, of the Memorial Sloan Kettering Cancer Center, has been the lead on this project, and she took some time at the 2016 International Mesothelioma Interest Group’s conference to speak to us about it.
When asked about the main differences in staging, Dr. Rusch outlined several, some of which are very technical and possibly mostly of interest to the treating physicians. One mentioned difference, however, revolved around a particular upcoming differentiation in the stage 4 disease. Once the new staging takes effect, some patients currently categorized as stage 4 will actually become stage 3b, a huge difference psychologically for the patient and their family, as well as the treating physician.
“For instance, right now, anything that’s stage T4 is considered stage 4 disease, and stage 4 disease for any patient automatically means ‘the end of the road.’ That’s now been moved to stage 3b, and only metastatic disease is stage 4,” said Dr. Rusch.
For a patient this can mean a significant change in terms of expected survival, but also in terms of availability of surgical therapeutic options, which are still available at stage 3, but not at stage 4.
To the question of whether patients diagnosed in the next six or so months should seek an updated staging come 2017, Dr. Rusch stated that that probably won’t be necessary as physicians will likely begin migrating to it soon.
“We as clinicians begin to implement in our minds and our practices new staging systems once they’ve been approved, but before they become official,” Dr. Rusch clarified.
“I think it’s important for patients to understand that this is an area in evolution. I think that the volumetric(**) study that we did and other studies along those lines will be incredibly important in selecting patients for therapy and assessing their response to therapy,” she concluded.
**Dr. Rusch is referring to a study currently in progress which compares more common measures for purposes of staging and treatment with the very precise volume measurements that aren’t yet standardized among centers. The goal is to make measurements as consistent as possible while also making sure they’re available in all clinics. We will keep you updated on the results of this study.